You’re in the middle of something great, things are heating up, and then—ouch. A sharp, stabbing sensation deep in your pelvis ruins the mood. If you’ve got a tilted womb, this probably sounds familiar. Honestly, it’s frustrating. About 20% to 25% of women have a uterus that leans backward toward the spine instead of forward toward the belly button. It’s not a disease. It’s just a body variation, like being left-handed or having blue eyes. But when it comes to intimacy, retroverted uterus sexual positions can be the difference between a night you want to remember and one you’d rather forget.
Deep penetration often hits the cervix or the ligaments surrounding a tilted uterus. This causes a specific kind of pain called deep dyspareunia. It feels heavy. Thumping. Sometimes it lingers as a dull ache long after you've finished.
Doctors often call this "atypical" anatomy, but for millions of people, it’s just their reality. Understanding how your body is shaped internally changes everything. It’s not about "doing it wrong." It's about the physics of your internal space. When the uterus tilts back, the ovaries and fallopian tubes often shift with it. This means they’re sitting right in the line of fire during certain movements.
Why Does a Tilted Uterus Even Matter?
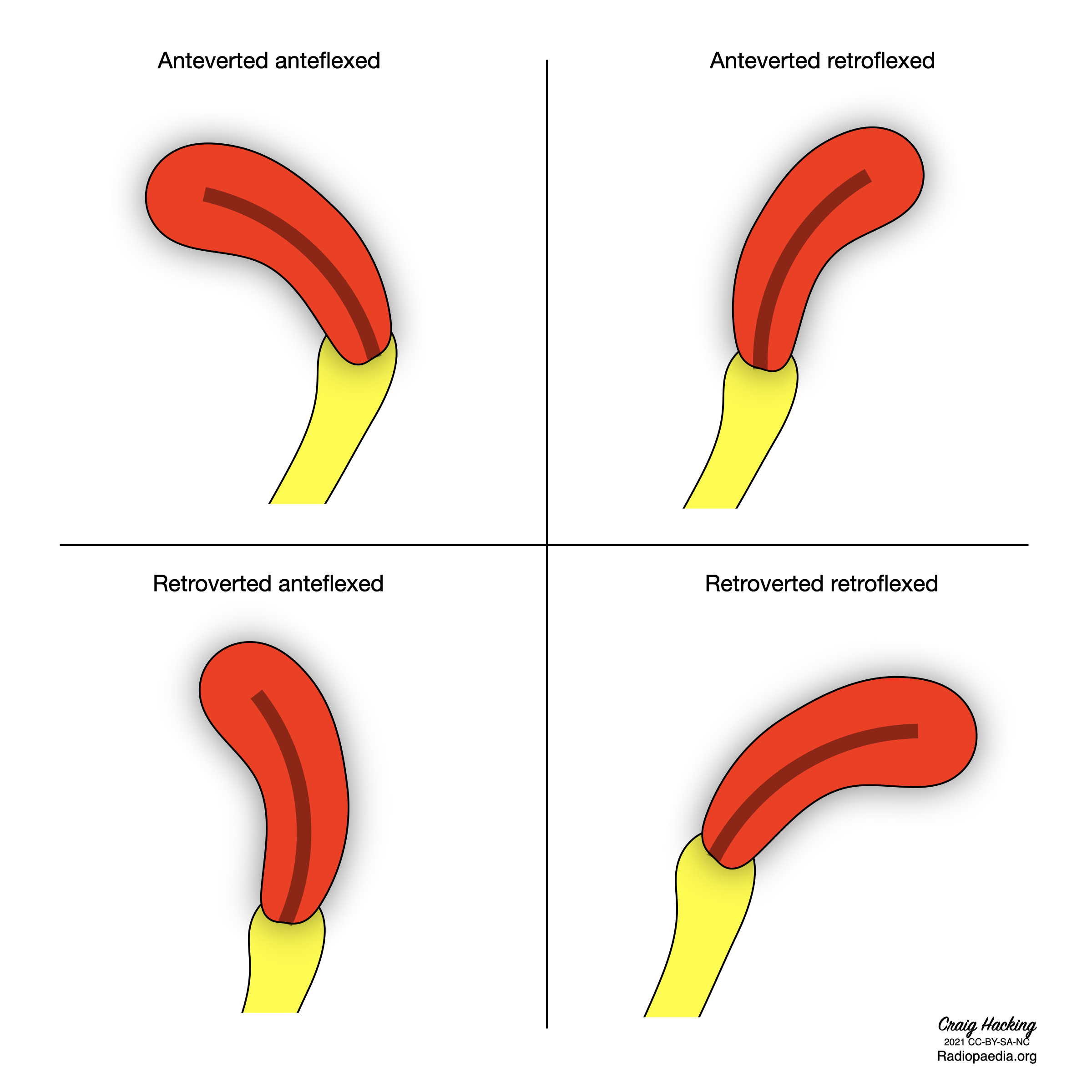
Basically, the uterus is held in place by ligaments. In a "standard" (anteverted) setup, the uterus sits like a little cap over the bladder. In a retroverted setup, it’s tipped toward the rectum. According to the American College of Obstetricians and Gynecologists (ACOG), this can be something you're born with, or it can happen later due to things like endometriosis, fibroids, or even pelvic inflammatory disease. Scar tissue—adhesions—can literally pull the organ backward and tether it there.
If your uterus is retroverted because of scarring, it’s usually less mobile. It can't "get out of the way" when things get intense. This is why some people find that certain angles feel like hitting a brick wall.
It isn't just about the uterus itself, though. The cervix is the gateway. When the uterus is tilted back, the cervix is angled differently in the vaginal canal. A direct "hit" to the cervix can trigger a vasovagal response in some people—feeling faint, nauseous, or just sudden, sharp cramping. Knowing which retroverted uterus sexual positions to avoid is just as important as knowing which ones to try.
🔗 Read more: Anterior Muscles of the Chest: Why Most Gym Rats Get Anatomy Wrong
The Problem With Traditional Entry
Doggy style is often the biggest offender.
Seriously.
Because of the angle of entry and the depth it allows, the penis or toy often makes direct, forceful contact with the retroverted fundus (the top of the uterus) or the sensitive ovaries. If you love this position but hate the pain, you have to modify the depth. It's a game of inches.
Missionary can also be tricky, but it's usually easier to fix. If your partner is lying completely flat on top of you, the angle of penetration is relatively straight. For a tilted womb, a straight shot isn't always the best shot. You want to create a "downward" slope or an "upward" curve to bypass the most sensitive spots.
Rethinking Retroverted Uterus Sexual Positions
Let’s talk about what actually works. The goal is to control depth and change the angle of the vaginal canal.
The Power of the Pillow (Modified Missionary)
Don't just lie there. Grab a firm pillow—or a dedicated wedge—and slide it under your hips. This is a game-changer. By elevating the pelvis, you’re essentially tilting your entire pelvic bowl. This can shift the uterus slightly forward or at least change the "point of impact" for your partner. It makes the vaginal canal more accessible while protecting the back-tilted cervix.
👉 See also: Regional One Health Elvis Presley Trauma Center: Why This Memphis Lifeline Is Still the Gold Standard
It feels different. More "shallow" in a way that actually feels better.
Side-Lying (The Spooning Method)
Spooning is underrated. Because you are both on your sides, penetration isn't as deep as it is in rear-entry positions. It allows for a lot of "grinding" or outer stimulation, which takes the pressure off the internal organs. If you have a retroverted uterus, the side-lying position allows the uterus to "fall" slightly to the side, often moving it out of the direct path of penetration.
Try it with your knees tucked up toward your chest. Then try it with your legs straight. The difference in sensation is wild.
On Top (Woman on Top)
This is the gold standard for anyone with pelvic pain. Why? Control. Pure and simple. When you're on top, you decide the depth, the speed, and the angle. If things get too deep or hit a "hot spot," you just lean forward or back to shift the trajectory.
Leaning forward while on top (sometimes called the Coital Alignment Technique or a variation of it) changes the internal geometry. It focuses sensation on the anterior vaginal wall (the G-spot area) and keeps the pressure away from the posterior fornix where a tilted uterus sits.
✨ Don't miss: Can You Actually Make Your Period Start Sooner? What Really Works
Modified Rear Entry
If you aren't ready to give up on rear-entry, try "The Frog." Instead of being up on your hands and knees, drop your chest all the way to the bed. Keep your hips up, but keep your upper body low. This "slope" changes the vaginal incline. Many people with a tilted uterus find this much more comfortable than the standard 90-degree angle of doggy style.
When Pain Is More Than Just Anatomy
It's kinky to talk about anatomy, but we have to be real: sometimes the tilt isn't the only issue. Dr. Mary Jane Minkin, a clinical professor at Yale School of Medicine, often points out that if sex is consistently painful, you shouldn't just "power through."
If you have a retroverted uterus and you also have heavy periods, painful bowel movements, or chronic pelvic pain, you might be looking at Endometriosis. In "endo," the uterus can become "fixed" or "frozen" in a retroverted position because of adhesions. In these cases, changing retroverted uterus sexual positions helps, but it won't fix the underlying inflammation.
Sometimes, the pain is actually "levator ani syndrome"—basically, the muscles of your pelvic floor are clenching in anticipation of pain. It’s a vicious cycle. You expect it to hurt, so you tense up, which makes it hurt more.
Communication and the "Ouch" Rule
You've got to talk. It's awkward at first, but explaining to a partner that "my uterus is basically a rebel that leans the wrong way" makes a difference. It turns a "you" problem into a "team" problem.
Use the "stoplight" system:
- Green: Everything is great.
- Yellow: It’s getting a bit deep/uncomfortable, slow down or change the angle.
- Red: Stop immediately.
Honestly, the mental stress of worrying about pain can kill your libido faster than the pain itself. Once you know which retroverted uterus sexual positions work for you, that anxiety starts to melt away.
Practical Steps to Better Sex with a Tilted Womb
Stop trying to make the "standard" positions work if they hurt. Your body isn't standard.
- Empty your bladder first. A full bladder takes up space and can push a retroverted uterus even further back, making it more sensitive to pressure.
- Focus on longer foreplay. This isn't just advice for the sake of it. When you're highly aroused, the "tenting" effect occurs—the vagina actually lengthens and the uterus lifts slightly higher into the abdomen. This can create a much-needed buffer zone.
- Invest in a "buffer" tool. There are products like the Ohnut (a series of stretchy rings) that go on the penis or toy to act as a depth limiter. It prevents deep "bottoming out" while still allowing for full, vigorous movement. It’s a lifesaver for people with a retroverted uterus.
- See a Pelvic Floor Physical Therapist. These experts are wizards. They can teach you how to relax the muscles around the uterus and even use manual techniques to improve the mobility of the organ itself.
- Check for "Fixed" Retroversion. If your doctor says your uterus is "fixed" (doesn't move when they push on it during an exam), you likely have scar tissue. This means positions that involve deep penetration from behind will almost always be uncomfortable, and you should prioritize shallow, face-to-face angles.
The bottom line is that a tilted uterus is just a structural quirk. It doesn't mean you're broken, and it definitely doesn't mean you're destined for a lifetime of mediocre or painful sex. It just means you have to be a bit more of an architect when it comes to your bedroom geometry. Move the pillows, change the incline, and don't be afraid to take the lead. Your body will tell you exactly what it needs if you're willing to listen and adjust the angle.