Death is the one thing we all have in common, yet we’re terrible at talking about how it happens. Honestly, it’s uncomfortable. But for thousands of Americans facing terminal diagnoses, the conversation isn't a philosophical exercise—it's a practical, urgent search for control. You’ve probably heard it called different things: physician-assisted suicide, medical aid in dying (MAID), or death with dignity. Whatever the label, the legal landscape for states that allow medically assisted death is a patchwork of strict regulations and shifting political winds.
Right now, if you live in Oregon, you have options that someone in Florida or New York simply doesn't have. It’s that blunt.
👉 See also: Red spots on scalp that itch: What’s actually going on with your skin?
Geography shouldn't determine how much pain you have to endure in your final weeks, but it does. As of 2026, the list of jurisdictions where this is legal has grown, but the barriers to actually accessing these laws remain incredibly high. People think you just sign a paper and it's done. That is a massive misconception. The process is grueling, bureaucratic, and intentionally slow.
The Current Map: Where is it Actually Legal?
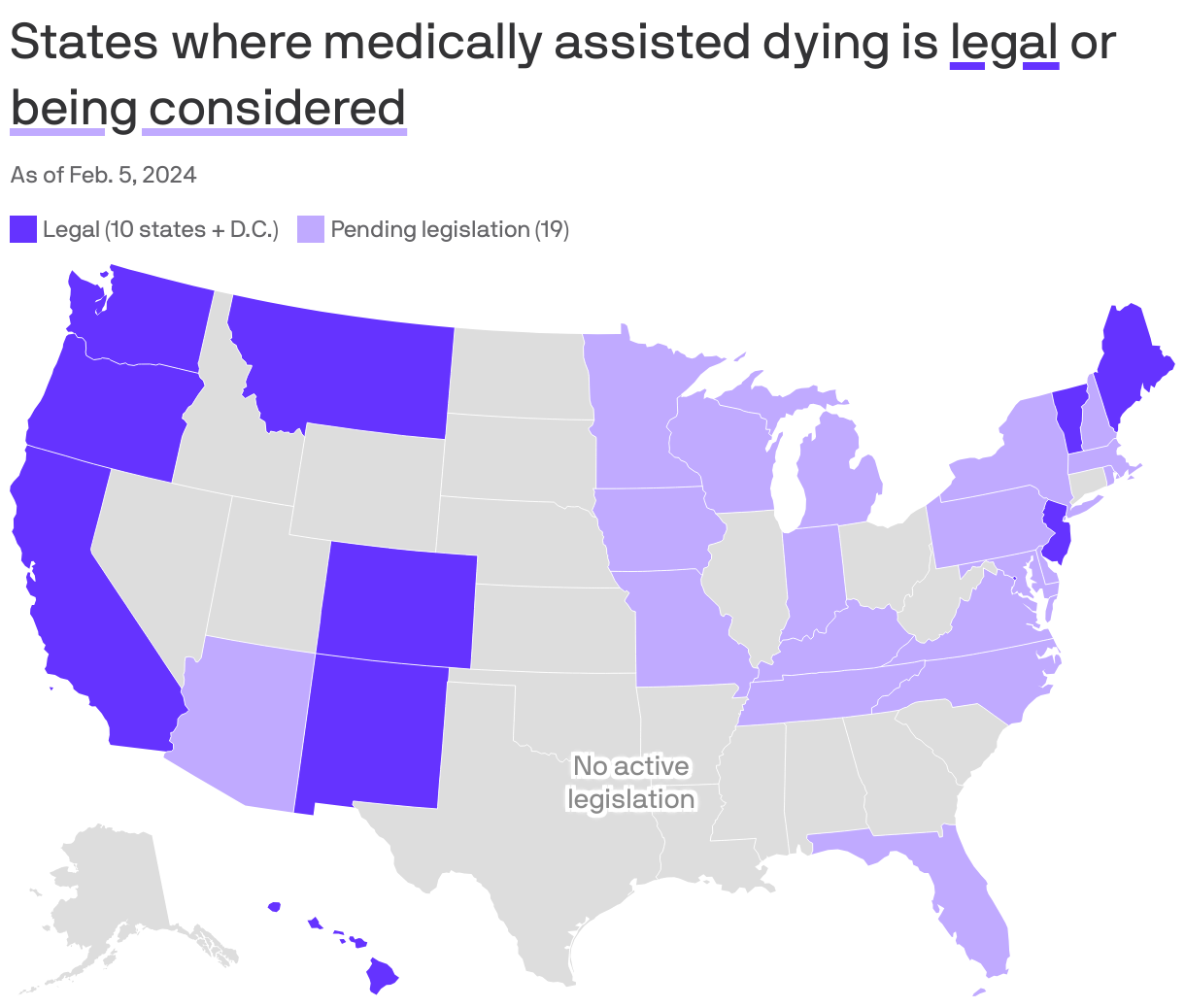
Currently, ten states and the District of Columbia have codified statutes allowing for medical aid in dying. Oregon was the pioneer, passing the Death with Dignity Act back in 1994. It took years of legal challenges before it finally went into effect in 1997. Since then, we've seen Washington, Vermont, California, Colorado, Hawaii, Maine, New Jersey, New Mexico, and the state of Washington follow suit.
Montana is the outlier. It’s a weird legal gray area there. In the 2009 case Baxter v. Montana, the State Supreme Court ruled that state law doesn't actually prohibit a physician from honoring a terminally ill, mentally competent patient's request for life-ending medication. So, while there isn't a specific "Death with Dignity" act on the books in Montana like there is in California, it's effectively shielded by judicial precedent.
The eligibility is usually the same across the board. You must be 18. You must be mentally competent. You must have a terminal prognosis of six months or less to live.
Most people don't realize how much the "residency" requirement is crumbling. For years, you had to be a resident of the state to use these laws. Oregon and Vermont recently settled lawsuits that effectively ended the residency requirement, meaning out-of-state patients can technically travel there for care. But let’s be real: traveling while you’re dying of stage IV cancer is a logistical nightmare that most people can't pull off.
It’s Not a "Quick Fix"
There’s this fear—often pushed by religious groups or disability rights advocates like those at Not Dead Yet—that these laws will be used to "coerce" people into dying. But if you look at the data from the Oregon Health Authority, the reality is the opposite. The safeguards are almost annoyingly robust.
First off, you usually need two separate oral requests, separated by a waiting period. Then a written request with witnesses. Then two different doctors have to sign off on your terminal status and your mental capacity. If there’s even a hint of depression clouding your judgment, they’re supposed to refer you for a psych eval.
Basically, you have to be dying, but you have to be "with it" enough to jump through a dozen hoops.
Wait. There’s more. You also have to be physically capable of self-administering the medication. The doctor doesn't give you a shot. They don't "put you to sleep." They write a prescription for a lethal dose of barbiturates or a compounded mixture, and you have to swallow it yourself. If you’re too weak to swallow or if you lose consciousness before you can take it, the option vanishes.
The Ethics and the Pushback
The American Medical Association (AMA) has long struggled with this. For a long time, their Code of Medical Ethics was flatly against it, stating that physician-assisted suicide is "fundamentally incompatible with the physician’s role as healer."
🔗 Read more: Why does my throat hurt all the time? What most people get wrong about chronic irritation
But the tide is turning.
Many state medical societies have moved to a position of "engaged neutrality." They realize that forcing a patient to suffer through a "bad death" might also be a violation of the "do no harm" principle. It’s a clash of two different definitions of harm. Is harm the act of ending a life, or is harm the act of allowing a person to waste away in agony against their will?
Critics like Dr. Ira Byock, a prominent palliative care physician, argue that we shouldn't need assisted death if we just did hospice and palliative care better. He’s got a point. Many people seek out states that allow medically assisted death not because they want to die, but because they are terrified of the dying process. They fear being a burden. They fear losing their dignity. They fear the pain that even morphine can't quite touch.
What the Data Actually Shows
If you dig into the annual reports from California or Oregon, the "typical" person using these laws isn't who you might expect. They are usually well-educated, have health insurance, and are already enrolled in hospice.
- Primary Diagnosis: Cancer is the big one, accounting for about 70-80% of cases.
- Top Concerns: Loss of autonomy, loss of dignity, and the inability to engage in activities that make life enjoyable.
- Unused Prescriptions: This is the most fascinating part. About one-third of people who go through the whole hassle of getting the medication never actually take it.
They just want the bottle on the nightstand. It’s an insurance policy. Knowing they could stop the pain if it becomes unbearable allows them to live more fully in the time they have left. It’s a psychological safety net.
The Cost of Dying
Let’s talk money, because it’s a factor people hate to admit. The drugs aren't cheap. After manufacturers jacked up the price of Seconal (secobarbital), many doctors moved to compounded mixtures of morphine, ethocyn, and diazepam. These can still cost between $500 and $1,000.
Most private insurance companies won't cover it. Medicare definitely won't cover it because it’s federal, and assisted death is still illegal at the federal level. Some state Medicaid programs cover it, but it’s a messy, state-by-state headache.
🔗 Read more: Full Body PEMF Mat: What Most People Get Wrong About Pulsed Electromagnetic Fields
And then there's the "opt-out" clause. Just because a state allows it doesn't mean your hospital does. Many Catholic-affiliated hospital systems—which make up a huge chunk of the US healthcare market—forbid their doctors from even discussing it. You could be in a legal state, in a room with a sympathetic doctor, and they still might be contractually barred from helping you.
How to Navigate the System
If you or a family member are looking into this, you can't wait until the last minute. You just can't. The timeline is your biggest enemy.
- Find a supportive doctor early. Don't assume your current oncologist will do it. Ask the question directly: "Do you participate in the Medical Aid in Dying law?"
- Verify your records. You need a definitive diagnosis and a clear "six months or less" prognosis in writing.
- Check your hospital’s policy. If your hospice provider or hospital has a religious affiliation, they might have a policy against MAID. You might need to transfer to a different facility or provider.
- Consult an advocacy group. Organizations like Compassion & Choices or the Death with Dignity National Center have patient navigators who know the local quirks of the law in each state.
The conversation is shifting. Every year, more bills are introduced in state legislatures. New York, Massachusetts, and Maryland are constantly on the verge of passing their own laws, but the political pushback remains fierce.
Actionable Next Steps
For those living in or considering moving to states that allow medically assisted death, there are concrete steps to ensure your end-of-life wishes are respected, regardless of whether you choose MAID.
- Complete an Advance Directive: This is a legal document that outlines your preferences for medical care if you become unable to speak for yourself. It’s different from a will.
- Appoint a Healthcare Proxy: Choose one person who knows your values and will fight for them when you can't. This person needs to be someone who won't crumble under pressure from other family members or doctors.
- Discuss "Voluntary Stopping of Eating and Drinking" (VSED): In states where MAID is illegal, VSED is a legal alternative that allows a competent person to hasten their death. It requires significant support from a hospice team but is an option in all 50 states.
- Document Everything: Keep a folder with your diagnosis, your doctor’s notes on your "mental capacity," and any written requests you make. In the legal world of assisted death, if it isn't written down, it didn't happen.
We are seeing a slow but steady move toward bodily autonomy in the final stages of life. While the legal map is still limited, the cultural shift toward "a good death" is becoming impossible to ignore. Understanding the specific hurdles in your state is the only way to ensure you actually have the choices you think you have.